![[VIDEO] Ultrasound-Guided Injection for Trigger Finger](https://drjordijimenez.com/imagen/100/100/Imagenes/infiltracion-ecoguidada-dedo-resorte-drjordijimenez.jpg)
- Home /
- PATHOLOGIES /
- SPINE PATHOLOGY /
- LUMBAR DISC HERNIATION
LUMBAR DISC HERNIATION
LUMBAR DISC HERNIATION
DR. JORDI JIMÉNEZ
The intervertebral disc can be divided into two parts: a gelatinous central part (nucleus pulposus) and a fibrous peripheral part (annulus fibrosus), which keeps the nucleus centered within the disc. Due to trauma or degenerative causes (most frequently), the annulus fibrosus can crack, creating a weak area through which the nucleus can shift toward the periphery, producing a disc protrusion or, if further progressing, a herniated disc (Figure 1).
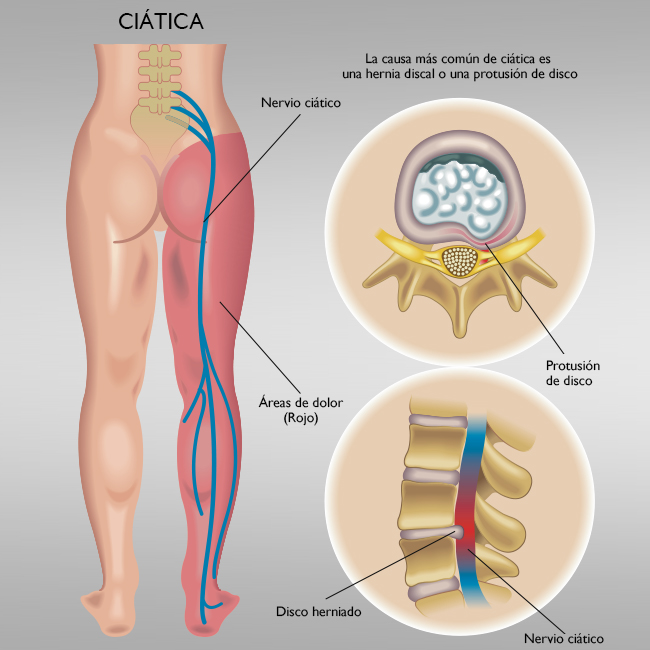
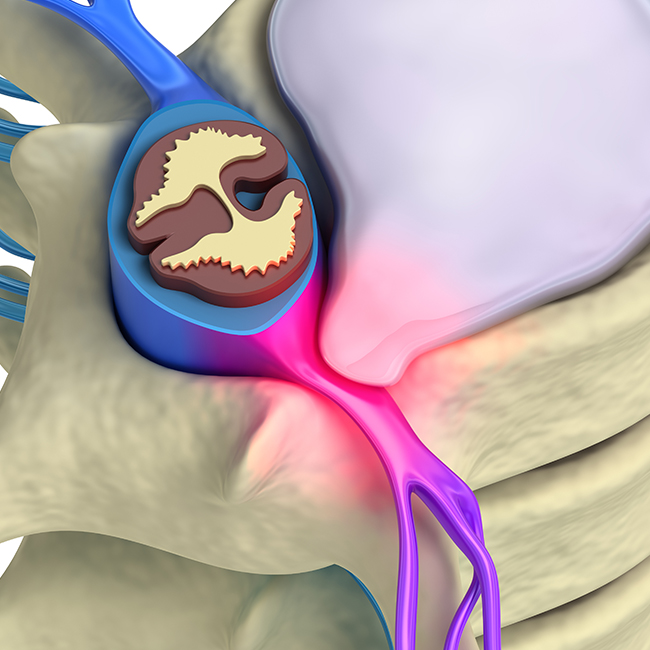
Figure 1
A herniated lumbar disc that causes compression of a nerve root, either due to its size or location, will cause the patient symptoms in the form of sciatic pain or sciatica. (Figures 1 and 2).

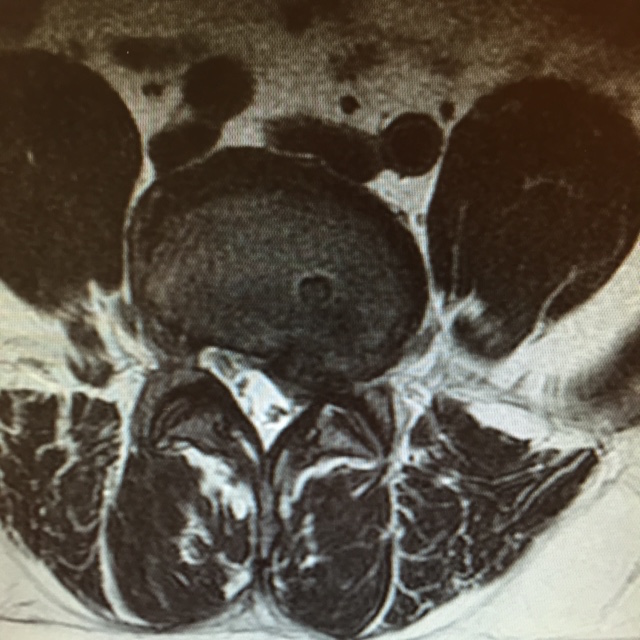
Figure 2.
Sciatica, or radicular pain, may be accompanied by sensory deficits (tingling, numbness, or altered sensation) or motor deficits (muscle atrophy, loss of strength, and deep tendon reflexes). These symptoms will vary depending on the lumbar level and the affected root.
The usual clinical picture is acute or subacute lumbar pain that limits the patient and radiates to a lower extremity, with a pain path dependent on the lumbar level of the affected root. It may be accompanied by altered sensation and/or motor disturbances (partial or complete loss of strength in knee or ankle mobility, depending on the injured root).
The specialist's interview and examination will be crucial for establishing a suspected diagnosis. Conventional radiology is not sufficient for diagnosing a herniated disc, but it will help rule out or confirm other possible problems.
The test that will identify the type of lumbar disc herniation, its location, size, and whether or not it compresses the nerve root is an MRI. In cases of associated neurological symptoms, electromyography will be very helpful, as it will determine the damage to the nerve root, if present (Figures 3 and 4).

Left extruded L4-L5 disc herniation .

Central extruded L5-S1 disc herniation .
Treatment for herniated discs is conservative in 80% of cases:
- repose
- analgesic-anti-inflammatory medication
- corticosteroid therapy, especially in the acute phase, and short-duration regimens.
After 6 weeks, if the pain remains intense, alternatives such as epidural blocks will be considered, and if these are not effective, surgical treatment will be considered .
Make an appointment with Dr. Jordi Jiménez. He'll see you in the center of Palma and help you regain your quality of life.
GENERAL TRAUMATOLOGY
SPORTS TRAUMATOLOGY
ULTRASOUND-GUIDED THERAPIES
IN PALMA DE MALLORCA
BLOG: TAKE CARE OF YOUR HEALTH
![[VIDEO] Ultrasound-guided infiltration of the lumbar facets](https://drjordijimenez.com/imagen/100/100/imagenes-pagina/sindrome-facetario-lumbar-drjordijimenez (1).jpg)
![[VIDEO] Ultrasound-guided infiltration of the hip joint](https://drjordijimenez.com/imagen/100/100/Imagenes/valgo-dinamico-rodilla-drjordijimenez.jpg)