Tietze Syndrome
- 30/11/2024
Acute chest pain is one of the most frequently seen conditions in an emergency department. Although some diseases that cause chest pain are potentially serious, in approximately 80% of cases the cause of chest pain is benign, and within this group, 20 to 50% are attributable to pain of musculoskeletal origin.
Obviously, we will focus on treating this musculoskeletal condition once other potentially serious pathologies of cardiovascular, pulmonary, or even gastrointestinal origin have been ruled out.
Musculoskeletal causes of chest pain can include bone or muscle trauma, overuse or repetitive movements, arthritis, fibromyalgia, infections, neoplasia, slipping rib syndrome, painful xiphoid syndrome, or Tietze's syndrome.
What is Tietze Syndrome?
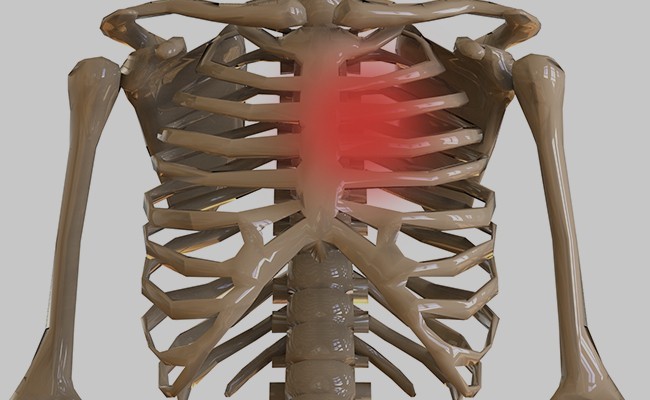
This article focuses on Tietze's syndrome, an inflammatory disease of the costochondral junction of unknown cause. Described by Tietze in 1921 as a benign, painful, non-suppurative swelling of the upper chondrosternal joint (the junction between the rib and the sternum).
It most commonly occurs in adults between 40 and 50 years of age, with a slight predominance in women.
Its cause is unknown; there are no established relationships between Tietze's syndrome and occupation, race, or geography. The few pathological studies vary from the absence of findings to degradation and inflammation of the costal cartilage.
How is Tietze Syndrome diagnosed?
Its main differential diagnosis is costochondritis, a condition characterized by tenderness and pain at the costochondral joints. In fact, the term costochondritis is often used interchangeably to refer to costosternal syndrome or chest wall syndrome, all of which involve chondrosternal or chondrocostal pain and tenderness, but without the swelling that characterizes Tietze's syndrome.
The diagnosis of Tietze's syndrome is made through a history and physical examination, which reproduces the pain by palpating the costochondral junction and the parasternal region. Provocative maneuvers such as the rooster-crowing maneuver or the crossed thoracic adduction test have also been described.
There are no specific radiographic findings or laboratory tests, but these complementary tests often help us rule out other diagnoses.
What is the treatment for Tietze Syndrome?
Treatment is always conservative, and the prognosis is usually favorable in the vast majority of cases:
- physical therapy.
- oral or topical anti-inflammatory treatment.
- in cases of persistent pain, ultrasound-guided corticosteroid injections are the basis of conservative treatment for Tietze's syndrome.
Book an appointment with Dr. Jordi Jiménez. He will see you at the center of Palma de Mallorca and help you regain your quality of life.
![[VIDEO] Ultrasound-Guided Injection for Trigger Finger](https://drjordijimenez.com/imagen/100/100/Imagenes/infiltracion-ecoguidada-dedo-resorte-drjordijimenez.jpg)
![[VIDEO] Ultrasound-guided infiltration of the lumbar facets](https://drjordijimenez.com/imagen/100/100/imagenes-pagina/sindrome-facetario-lumbar-drjordijimenez (1).jpg)
![[VIDEO] Ultrasound-guided infiltration of the hip joint](https://drjordijimenez.com/imagen/100/100/Imagenes/valgo-dinamico-rodilla-drjordijimenez.jpg)